TL;DR:
Microplastic diagnostics in humans: ‘The 3Ps’ Progress, problems, and prospects” by Gurusamy Kutralam‑Muniasamy, V.C. Shruti, Fermín Pérez‑Guevara and Priyadarsi D. Roy is a deep dive into how scientists actually detect microplastics in human bodies, what we’ve found so far (from blood to placenta to feces), why contamination and methods are a minefield, and where human microplastics research needs to go next.
What this review is about
This 2023 review pulls together everything we currently know about microplastics in human biological samples – think blood, lungs, liver, placenta, breastmilk, sputum, colon, feces and more. The authors systematically screened thousands of papers and narrowed it down to 20 high‑quality studies that actually identified polymers using robust techniques like FTIR, Raman, Py‑GC–MS or HPLC‑MS/MS. Their goal is to map the 3 Ps: progress, problems and prospects in “microplastic diagnostics” in humans.
Progress: where we’ve got to
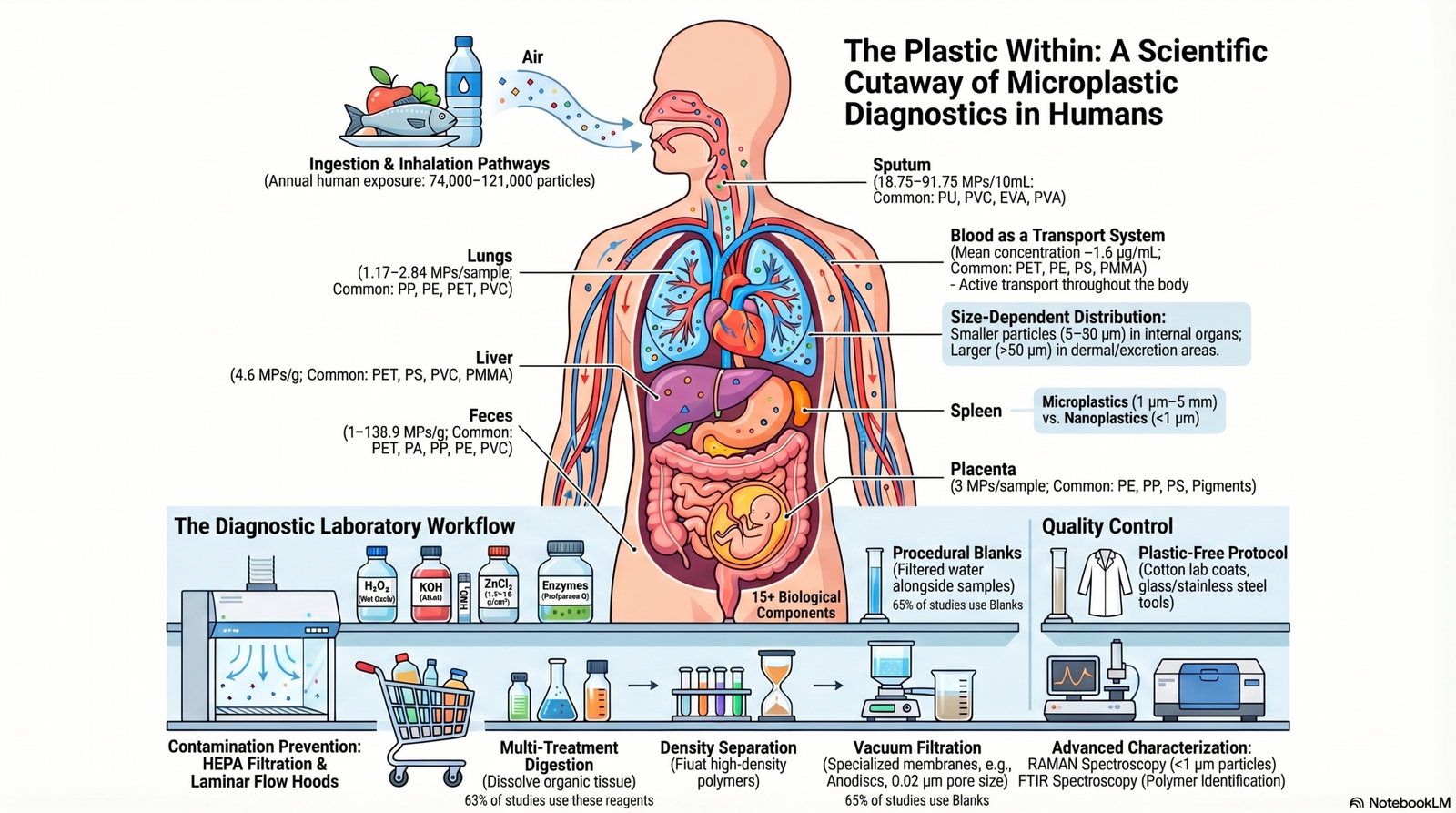
The first paper on microplastics in human samples only appeared in 2019, but most of the selected studies were published in 2021–2022 – this field is exploding. Researchers have now reported microplastics in at least 15 human matrices, including blood, lung, liver, spleen, placenta, meconium, breastmilk, colon, saliva, sputum, hair, skin, hands and feces. Feces is the most commonly studied sample because it’s non‑invasive and gives a snapshot of gut exposure.
On the lab side, the paper walks through the full diagnostic pipeline:
- Sampling: invasive (tissues, blood, BALF) vs non‑invasive (saliva, hair, skin, feces, breastmilk)
- Digestion & isolation: combinations of H₂O₂, KOH, NaOH, HNO₃, enzymes and density separation (CaCl₂, ZnCl₂) to strip away organic matter without destroying plastics
- Detection: Raman and FTIR spectroscopy, Nile Red staining, Py‑GC–MS and HPLC‑MS/MS, often in combination for polymer ID and size distribution
Raman is emerging as a workhorse because it can detect particles below 1 μm, which matters when we care about particles small enough to cross cell membranes.
What’s actually in us?
Across the 20 studies, microplastics were detected in almost all sample types, with 0–100% prevalence depending on organ and study design. Reported mean levels (very rough baseline numbers) include: about 1.6 μg/mL in blood, a few MPs per gram in placenta, meconium, liver and lung, and from roughly 1 to 139 particles per gram in feces. Shapes are mostly fibres and fragments, dominated by transparent/white and blue particles; sizes range from ~700 nm up to 5 mm, with smaller particles (<50 μm) turning up more in internal tissues and larger ones in skin, hands, hair and stool.
Polymer types span the usual suspects – PET, PE, PP, PVC, PS and a long list of engineering and specialty polymers – with over 45 plastic types reported in human samples. Some studies link polymer signatures in tissues to what people actually eat and use (e.g., food, drinking water, personal care products), underlining that ingestion and inhalation from multiple sources are feeding the body burden.
Intriguingly, some papers report higher microplastic loads in diseased tissues (e.g., cirrhotic liver, lung nodules, inflammatory bowel disease) than in healthy controls, but the review stresses we don’t yet know if plastics contribute to disease, or if disease simply makes retention easier.
Problems: contamination and lack of standards
The “problems” section is a reality check for microplastics‑in‑humans headlines. Cross‑contamination is everywhere: fibres from air, lab coats, masks, filters and plastic labware can easily fake a signal. Many studies use blanks, but often only visually, without full polymer ID, and some show the same polymers in blanks and samples – at least 30% of studies in this review were clearly affected by contamination issues.
- Contamination‑control practices (clean rooms, HEPA‑filtered air, laminar flow hoods, plastic‑free protocols) are highly inconsistent.
- Extraction chemistries like 65% HNO₃ can damage polymers and under‑estimate real loads.
- Recovery tests are rare outside feces and blood, so we often don’t know how much we’re losing.
There is no standard method yet for any human matrix, which makes cross‑study comparison very shaky.
Prospects: what needs to happen next
In the “prospects” section, the authors outline a research roadmap. Priorities include:
- More and larger biomonitoring studies outside Europe and Asia, including far more work on children and vulnerable subgroups.
- Longitudinal follow‑up of patients with documented microplastic loads in tissues, to see how levels change and whether they track disease.
- Better, standardized contamination‑control protocols and recovery experiments for every matrix.
- Deeper toxicology on microplastics and their co‑contaminants, plus an urgent push into nanoplastics, which animal work already shows can be absorbed and excreted in urine.
- Translating all this into clear public communication, not just specialist papers.
The big message: microplastics in humans are real, globally relevant, and technically challenging to measure – and we’re only at the start of building reliable diagnostics that can link exposure to real health outcomes.
Leave a Reply